In 2009, for the first time, U.S. deaths linked to drug abuse exceeded those caused by road accidents (see chart), according to the Federal agency of the U.S. Government "Centers for Disease Control and Prevention ", which in 75% of cases points the finger at the inappropriateness of prescriptions. The main cause of medicines abuse is the dependence on analgesics in the opioid family. These are in fact the category of drugs most prescribed in the United States and in the last ten years the number of units prescribed has almost quadrupled. The major problem is that often their side effects or the risks associated with an out-of-control use of these drugs has been underestimated.
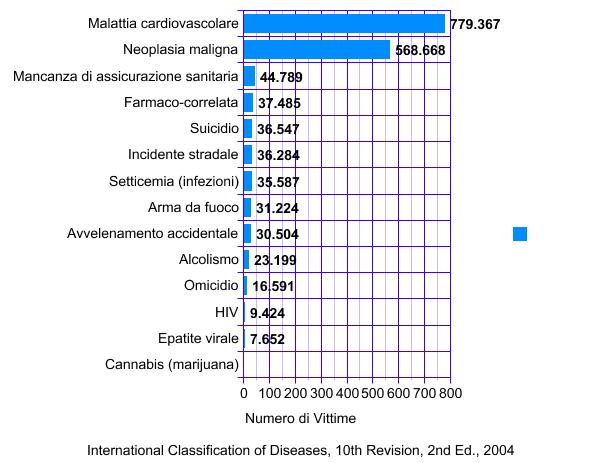
"Drug-related" includes both legal and illegal substances. In the period 1999-2008
rates of death by overdose, sales and hospitalization
linked to the abuse of opioid analgesics (OPR= opioid pain reliever)
increased significantly. Compared to 1999, in 2008 the number of
deaths from drug overdoses nearly doubled. Similarly, sales of
opioids quadrupled in 2010 compared to 1999 data.
(Source: Centers for Disease Control and Prevention).
Until 15 years ago, these drugs were almost exclusively used for the treatment of pain in the postoperative phase or in terminal cancer patients. It was precisely on the basis of the good results obtained in controlling pain in those cases, that opioids began to be prescribed to patients suffering from chronic pain. This most recent use prompted pharmaceutical companies to propose new, targeted formulations. Sales, last year, reached $ 8.5 billion, twice the figures reached in 2001 (data: IMS Health). The situation is truly alarming also due to the recreational use, especially by adolescents, of drugs such as oxycodone, developed to alleviate the most intense forms of pain, but increasingly involved in a growing illicit trade.
Something however is changing and the lead State this time is that of Washington, which placed limits and stricter controls on the prescription of pain medications - a significant and difficult change not only for patients, but also for physicians. Indeed the battle has to be fought mainly in hospitals and in practitioners' offices, rather than in the street. What is often left unsaid, like a taboo, is that it is the doctors who overdo with prescriptions, giving in to the pressing demands of patients who have developed an addiction. The risks of using painkillers include sleep apnea, falls and bone fractures in the elderly but, in extreme cases, death by overdose. For this reason, legislators in the Washington State, last year imposed new requirements on physicians prescribing opioids. The Centers for Disease Control and Prevention invited them to be more cautious when prescribing them, emphasizing that just in 2008 overdose deaths were 14,800. It is indeed paradoxical that a practice that was started to relieve patients' pain ends up even causing their death.
The analysis of the files of patients who died from overdose shows failure to perform the required drug tolerance monitoring by physicians. Often those who suffer from chronic pain are affected by concomitant conditions that need special attention (anxiety, depression) and that do not improve by simply increasing the drug dosage. Several scientific studies have since shown the risks associated with the abuse of opioid drugs which, for example, suppress the production of sex hormones, altering the physiology of patients well beyond the mere sexual sphere. Other research highlighted the benefits of alternative, non-pharmacological therapies, effective in many cases. However, despite the heated debate and the accusations of "cruelty" (from patient groups, pharmaceutical companies and insurance companies), in the State of Washington a law was passed establishing a threshold in the dosage of medication prescribed (equivalent to 120 milligrams of morphine per day), above which the use of a commission of experts is activated.
Physicians will certainly need to follow specific training courses to be able to judge which molecule and what dosage to prescribe and for which indication, in addition to learning how to handle cases of dependency and abstinence.Among the professionals most at risk of error there are, undoubtedly, emergency doctors who often have neither the time nor the means to judge whether the patient who is complaining, for example, of a terrible toothache is telling the truth. When in doubt, the doctor prescribes the drug, because a denied prescription in cases of genuine necessity becomes the basis for an .adverse evaluation of the work of the professional. A research conducted by the National Hospital Ambulatory Medical Care Survey showed that from 1997 to 2007, painkillers were prescribed in 3 cases out of 4 during a visit to the dental emergency room and that the number of prescriptions related to toothache in this type of departments increased by 26%.
An
even more worrying area is that of the Maternity Departments which have seen
an increasing number of women addicted to opioids and,
consequently, of infants showing withdrawal symptoms. A
study published in the Journal
of the American Medical Association
quantified the phenomenon and the costs related to it: in the U.S.
every hour a child is born with symptoms of "Neonatal withdrawal syndrome",
therefore, on average, 13,500 infants a year suffer from
the consequences of the abuse of painkillers inappropriately used
by their mothers. From 2000 to 2009 the number of this type of
women giving birth has increased fivefold and the average cost related to assistance
given to their children exceeds 53 thousand dollars for each case.
Symptoms include seizures, respiratory problems,
dehydration, feeding difficulties, tremor and irritability.
These children need long term care and specific therapies based on
methadone and morphine. The worst news is that as of today we do not know
whether any lasting effects can be envisaged for these children
over time.Obviously the best thing is to
prevent the mother's problem, helping her in treating the
addiction to drugs before birth or, better yet, before
pregnancy.
A special medical help is even coming from a video game designed by
scholars of the Faculty of Medicine of Northwestern University and
developed by engineers at Johns Hopkins University, which uses
a technology similar to that used by the FBI to train its agents
for interrogation techniques. The video game will help doctors
recognize the symptoms of opioid dependence during the
interview with the patient, with a series of guided questions and answers.
However, while overseas the measures (legislative, and not only) to to fight the abuse of opioids increase, in Italy the situation is quite different and the culture of pain shows peculiarities in some respects even opposite. In March 2010 a law came into force, unanimously passed earning the applauses of the whole Parliament, with the intent of promoting "hospitals with no pain". A little over a year after its enactment, in July 2011, a survey promoted by the Senate Investigation Commission on the National Health Service was carried out to verify its effective implementation throughout the country. Well, hospitals and physicians throughout the country ignore or only partially apply the law. The right not to suffer for millions of Italian is essentially guaranteed only in the North and partly in the Centre of Italy, while the South is lagging behind. From Rome down, the use of opioids is left at the starting post: since law 38/2010 has authorized doctors to use a regular prescription form to prescribe them, their consumption grew too little (7% in a year), compared to the already little number of units sold in the past which make Italy one of the key laggards in Europe. The survey, conducted in 244 hospitals (86 in the North, 103 in the Center, 55 in the South) used a check-list prepared to verify, among other things, whether there were any committees or programs in place for pain control, palliative care units, the use of forms for evaluating acute and chronic pain, information material for patients and an active communication network with general practitioners. The average compliance with the requirements set by the law was 71% with peaks of 88% in the North, 75% in the Centre and 53% in the South, where, however, at least 5 regions do not reach 50%. These results show insufficient compliance with the obligations imposed by law.But above all, they unveil a widespread cultural lag with respect to the attention paid to pain in Italian hospitals : an issue that requires urgent consideration and action.

