Prof. Hans Bärlocher left the hospital after a long working day. Outside the building, he took a deep breath of fresh Spring air; then, he smelled his right hand. Yes, it had the faint, but typical copper smell. This reassured him that he had not pick up any germs when going through the series of doors to leave the clinic. All the doors in his hospital had recently been refitted with door handles and push plates of antimicrobial copper. Also, many other items of stainless steel, like trays, bed rails, bathroom fixtures or toilet seats had been replaced by corresponding objects made of copper - and finally, after years of rise, hospital acquired infections were declining again in his hospital.
In spite of clean, modern facilities, hospital-acquired, or nosocomial, infections are on the rise in most other institutions across the world. In the last surveillance report of the EU, three million nosocomial infections were reported, resulting in a death toll of 50,000 per year. Often, these infections are due to highly antibiotic-resistant microorganisms, like methicillin-resistant Staphylococcus aureus, referred to as MRSA. Live MRSA can readily be detected on many surfaces in a hospital and are particularly abundant on frequently touched objects like keyboards, pens, bed rails or desk surfaces (Fig. 1). It has been shown in one study that mobile phones are heavily contaminated with bacteria and MRSA could be isolated from 52% of the mobile phones tested (1). Whether the infection of patients occurs directly from such contaminated surfaces or by other routes is not clear, but contaminated surfaces clearly provide a reservoir of infectious bacteria. The fact that there is a significant risk of dieing in the hospital by a hospital-acquired infection is frightening and requires urgent action. But what can be done, in addition to the already very stringent hygiene concepts? Is copper the answer?
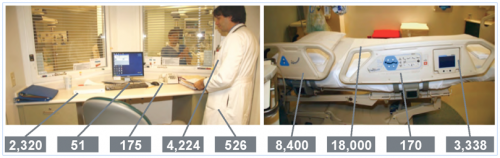
Fig. 1. Number of bacteria, in colony forming units
per 100 cm2, found on various surfaces in a hospital ward.
The use of copper in medicine is not new. Medical applications of copper were already described in the Egyptian Smith Papyrus, written between 2600 and 2200 BC. This medical text details the application of copper to sterilize chest wounds and drinking water (2). Greeks, Romans, Aztecs, and others also used copper or copper compounds for the treatment of ailments burns, intestinal worms, ear infections, and for hygiene in general. In the 19th century, new awareness of copper’s medical effects was raised by the observation that copper workers did not contract cholera in the 1832 and subsequent cholera outbreaks in Paris. The use of copper in medicine became widespread in the 19th and early 20th century and a variety of inorganic copper preparations were used to treat chronic adenitis, eczema, impetigo, tubercular infections, lupus, syphilis, anemia, chorea, and facial neuralgia (2). The medical use of copper continued until the advent of commercially available antibiotics in 1932. The spread of antibiotic resistance through selective pressure began and today has made antibiotic resistant bacteria like MRSA ubiquitous and a major cause of nosocomial infections. This has raised the need for new approaches to keep pathogenic microorganisms at bay.
Recent scientific studies clearly showed that copper and copper-containing alloys rapidly kill bacteria, yeasts and viruses on their surface (3). This called for the re-introduction into the hospital of copper, brass, bronze, and other alloys rich in copper to create antimicrobial surfaces. The so called 'contact killing' on copper-containing metal surfaces is very rapid and complete. Ten to a hundred million bacteria are killed per minute, and no live microorganisms can generally be recovered from copper-containing surfaces after prolonged incubation. Over a dozen species of bacteria, yeast and viruses have been shown to be killed on copper and copper alloy surfaces. This is in stark contrast to stainless steel. On this clean-looking material, microorganisms survive for days or even weeks. They gather in microscopic scratches and are impossible to remove by standard cleaning techniques (Fig. 2).
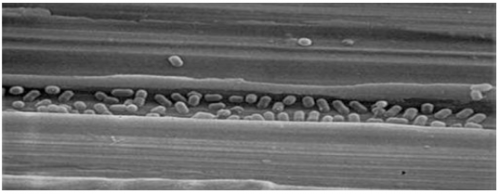
Fig. 2. Bacteria in a scratch on a
stainless steel surface.
The antimicrobial activity of copper is now established and copper has recently been registered at the U.S. Environmental Protection Agency as the first solid antimicrobial material (http://www.antimicrobialcopper.com). Copper and its alloys are thus poised to become a standard addition to the established hygiene procedures of hospitals. In a number of hospitals around the World, copper is now being evaluated for use on touch-surfaces such as bathroom fixtures, toilet seats, and bed rails, in the attempt to curb nosocomial infections (Fig. 3). All of these studies are still ongoing, but preliminary results look very promising. In a study published by the University Hospitals Birmingham, the numbers of microorganisms on the surfaces of copper-containing items were reported to be 90% to 100% lower than on equivalent control surfaces (4). However, longer study times are necessary to assess if these antibacterial effects also curb the frequency of nosocomial infections.
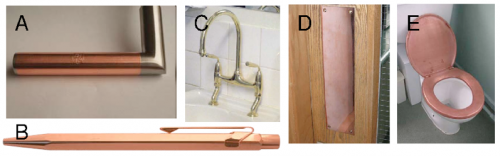
Fig. 3. Antimicrobial copper items
for use in hospitals: A, self-sticking copper foil to apply to critical places
from copper-protect.de; B, CopperPenâ for doctors and nurses from
copperpen.ch; C, brass fixture for sinks; D, copper push plate for doors; E,
copper toilet seat.
What is the mechanism of contact-killing of bacteria by copper? As a first step, the contact of bacteria with the copper surface ruptures the membrane by an unknown mechanism (Fig. 4). This leads to the loss of cell content. Large amounts of copper ions dissolved from the metal surface are then taken up by the cell. The dissolved copper ions react with oxygen, thereby forming so called reactive oxygen species. These are radicals like OH۬·, which can react with biomolecules of a cell and cause severe damage. Finally, the DNA is fragmented into small pieces which seep out of the cell. This sequence of events is still tentative, but it is already clear that the killing of bacteria by copper involves several mechanisms.

Fig. 4. Schematic representation of the
events in contact-killing. Copper ions dissolved from the copper surface causes
cell damage (A), the cell membrane ruptures, leading to loss of the cell
content (B), copper ions lead to the generation of toxic radicals which cause
further damage (C), and DNA becomes degraded and leaves the cell (D).
But if copper kills bacteria, is it not dangerous to me? No! Copper is not taken up significantly through the skin, so touching copper, brass or bronze is never a risk. But the contact of the skin with copper does lead to the generation of the copper smell, which had reassured Hans Bärlocher that the door handles in his hospital were indeed out of copper or brass. The smell arises from traces of aldehydes which form when copper comes into contact with skin. For unknown reasons, our nose is exquisitely sensitive to these compounds, but they are of no concern. Importantly, copper is an essential trace element, so your body needs copper. If anything, you may be endangered of having too little copper. All food contains some copper, but particularly copper-rich food like liver, shellfish or nuts may be missing in your diet. Also, the copper content of your drinking water can vary greatly, from nearly undetectable copper to over 1 mg per liter. Unfortunately, there is no method to determine if an individual has enough or too little copper, but most scientists would agree that one cannot consume too much copper with a normal diet. However, a US company advances the concept that copper in the drinking water is a risk factor for Alzheimer disease and they call this copper "dangerous free copper" (see http://www.anticopper.com). This is an extreme standpoint for which there is no conclusive data.
Will there soon be superbugs which have become resistant to contact-killing by copper surfaces? Or are there bacteria which are naturally refractory to contact-killing by copper? Live bacteria can in fact be isolated from copper-containing surfaces. In a recent study, live bacteria were isolated from European 50-cent copper coins. However, when re-tested, all the bacterial strain were sensitive to contact-killing by copper (5). Apparently, survival of bacteria on copper is enabled by patches of dirt, emphasizing the need for rigorous cleaning of antimicrobial copper surfaces. No superbug naturally resistant to copper could so far be isolated. But could it emerge in the near future? Several arguments speak against it: First, the genetic material of bacteria is completely degraded during contact-killing, preventing the transfer of resistance genes to other organisms (6). Secondly, contact-killing is very rapid and cells are not dividing on copper surfaces, precluding the acquisition of resistance, and finally, copper and copper alloys have been used by humans for thousands of years, yet, no bacteria fully resistant to contact-killing have been discovered.
Clearly, copper surfaces are a welcome new means in the fight against hospital acquired infections. However, copper cannot replace any of the standard hygiene practices already in place and it will not be the sole measure to get a grip on nosocomial infections. Many additional measure like pre-screening of patients and staff for MRSA, quarantine of newly admitted patients etc. must also be considered, although these may be far more costly then the use of antimicrobial copper.
Acknowledgment
The author is supported by the Swiss
National Foundation and the Swiss State Secretary for Education & Research.
1. Ulger,
F., Esen, S., Dilek, A., Yanik, K., Gunaydin, M., and Leblebicioglu, H. (2009) Ann. Clin. Microbiol. Antimicrob. 8, 7.
2. Dollwet, H. H. A. and
Sorenson, J. R. J. (1985) Trace Elements
in Medicine 2, 80-87.
3. Grass, G., Rensing, C., and
Solioz, M. (2011) Appl. Environ Microbiol.
77, 1541-1547.
4. Casey, A. L., Adams, D.,
Karpanen, T. J., Lambert, P. A., Cookson, B. D., Nightingale, P., Miruszenko,
L., Shillam, R., Christian, P., and Elliott, T. S. (2010) J. Hosp. Infect. 74,
72-77.
5. Espirito Santo, C., Morais,
P. V., and Grass, G. (2010) Appl.
Environ. Microbiol. 76,
1341-1348.
6. Warnes, S. L., Green, S. M.,
Michels, H. T., and Keevil, C. W. (2010) Appl.
Environ. Microbiol. 76,
5390-5401